

Introduction: Allogeneic hematopoietic cell transplantation (HCT) can be employed as curative therapy for many non-malignant diseases but there is risk of transplant related complications. Pre-HCT, patient-specific factors can help inform risk using the HCT comorbidity index (HCT-CI); however, it can be difficult to apply in children and young adults, where assessment of organ function differs from those defined by the HCT-CI. We aimed to supplement the HCT-CI with pediatric-specific comorbidity definitions to broaden the use of the HCT-CI for pediatric & young adult patients with non-malignant diseases.
Methods: Patients <40 years old (yo) who received first allogeneic HCT for non-malignant diseases from 2008-2017 were identified in the Center for International Blood and Marrow Transplant Research (CIBMTR) database. Separate training and validation samples were created using a 2/3, 1/3 split. Adjustment to the definition of renal disease was made, supplementing with estimated glomerular filtration rate (eGFR) and defined as mild (60-89) or moderate/severe (<60ml)/min/1.73m2. Nutritional assessment was supplemented to include obesity (body mass index (BMI) >95th percentile for <18yo) and added assessment of underweight (BMI <5th percentile for <18yo, <18kg/m2 for ≥18yo) by CDC guidelines. History of mechanical ventilation was included as an additional marker of pulmonary disease. Multivariable Cox regression analyses assessed the effect of each comorbidity, and then the modified scores, on overall survival (OS), adjusting for age, primary disease, donor, performance status, recipient CMV status, and year of HCT. We propose 2 potential scores based on modifications for pediatric and young adult patients: 1) Expanding the HCT-CI with broader definitions that can be applied to younger patients, 2) Simplifying the HCT-CI to remove certain comorbidities with hazard ratio (HR) <1.2. C-statistic was used to compare the modified scores to the original HCT-CI.
Results: 2,815 patients received allogeneic HCT for non-malignant diseases (25.8% aplastic anemia, 26.5% immune deficiency, 18.2% hemoglobinopathies, 29.5% other) at a median age of 6 (<1-39)yo. 84.3% were ≤18yo and 15.7% were 19-40y. Conditioning intensity was myeloablative in 48.5%, donors were primarily matched sibling (21.2%) or well-matched unrelated donors (25.6%), and bone marrow was primary graft source (54%). Using the original HCT-CI, patients were categorized with scores of 0 (59%), 1-2 (20.8%), and ≥3 (20%).
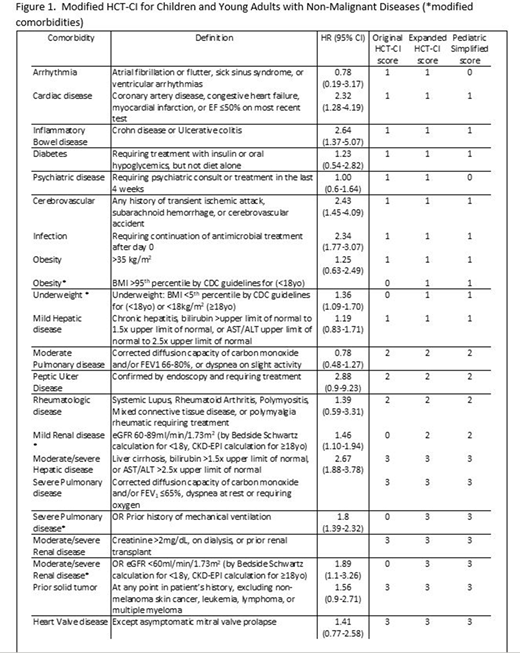
In multivariable analysis, comorbidities with pediatric-specific definitions demonstrated increased hazards of death, including in underweight patients (HR 1.55, 95% confidence interval (CI) 1.18-2.04), those with history of mechanical ventilation (HR 1.85, 95%CI 1.39-2.48), mild renal disease by eGFR (HR 1.49, 95%CI 1.11-2.0), or moderate/severe renal disease by eGFR (HR 2.04, 95%CI 1.1-3.26). Therefore, comorbidities were expanded to include these definitions in the Expanded HCT-CI. Expanding the comorbidity definitions increased the number of patients identified as having pre-HCT comorbidities: 35% were categorized with scores of 0, 32% with scores of 1-2, and 33% with scores of ≥3. Figure 1 shows the expanded comorbidity definitions and effect on OS. Arrhythmia and Psychiatric diseases were noted to have HR <1.2 and were removed in the Pediatric Simplified score. Increasing scores had increasing risk of death in the Expanded HCT-CI [validation cohort HR 1.31, 95%CI 0.81-2.02 for scores (1-2), HR 2.03, 95%CI 1.34-3.07 for (≥3), compared to scores of 0] and the Pediatric Simplified score (validation cohort HR 1.34, 95%CI 0.89-2.02 (1-2), HR 1.97, 95%CI 1.82-2.93 (≥3), compared to scores of 0]. Modifications to the HCT-CI predicted outcomes similar to the original HCT-CI (validation cohort c-statistic at 2yr - HCT-CI 64.3, expanded HCT-CI 65.8, and pediatric simplified HCT-CI 65.8).
Conclusion: Modifications to definitions in the HCT-CI can create a pre-HCT risk tool that more broadly classifies organ dysfunction for children & young adults. By expanding the comorbidity definitions, 24% more patients were re-categorized as having at least 1 comorbidity, allowing for better assessment of pre-HCT risk. This expanded HCT-CI performs as well as the HCT-CI but is more broadly applicable to children & young adults with non-malignant diseases and can aid physicians in pre-HCT counseling.
Schiller:Johnson & Johnson: Current equity holder in publicly-traded company; Karyopharm: Research Funding; Sangamo: Research Funding; AstraZeneca: Consultancy; Amgen: Consultancy, Current equity holder in publicly-traded company, Research Funding, Speakers Bureau; Agios: Consultancy, Research Funding, Speakers Bureau; Incyte: Consultancy, Research Funding, Speakers Bureau; Novartis: Consultancy, Research Funding; Ono Pharma: Consultancy; Celgene: Research Funding, Speakers Bureau; Sanofi: Speakers Bureau; Gilead: Speakers Bureau; Stemline: Speakers Bureau; Onconova: Research Funding; Samus: Research Funding; Regimmune: Research Funding; Pfizer: Current equity holder in publicly-traded company, Research Funding; Cyclacel: Research Funding; Daiichi Sankyo: Research Funding; Deciphera: Research Funding; DeltaFly: Research Funding; Bristol-Myers Squibb: Current equity holder in publicly-traded company, Research Funding; Forma: Research Funding; FujiFilm: Research Funding; Gamida: Research Funding; Genentech-Roche: Research Funding; Geron: Research Funding; Jazz Pharmaceuticals: Research Funding; Kite Pharma: Research Funding; Mateon: Research Funding; MedImmune: Research Funding; Tolero: Research Funding; Trovagene: Research Funding; Kaiser Permanente: Consultancy; Celator: Research Funding; Constellation: Research Funding; Astellas Pharma: Honoraria, Research Funding; Ariad: Research Funding; Actinium: Research Funding; Abbvie: Research Funding. Stadtmauer:Amgen Inc, Celgene Corporation, Janssen Biotech Inc, Novartis, Onyx Pharmaceuticals, an Amgen subsidiary, Takeda Oncology: Consultancy. Pasquini:Bristol Myers Squibb: Consultancy; BMS: Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Other; Novartis: Research Funding; Kite: Research Funding. Thakar:Infectious Disease Research Institute: Consultancy. Sorror:Jazz Pharmaceutical: Other: Honorarium for Advisory role. .

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal